
一例ECMO治疗相关DIC的日本案例
成功救治一例长期使用静脉-静脉体外膜肺氧合(ECMO)的八旬患者
Successful management of prolonged venovenous extracorporeal membrane oxygenation in an octogenarian
昭和大学东京东洋病院心血管外科
Masami Takagaki · Hiroki Yamaguchi ·Shinichi Mitsuyama· Tasuku Kadowaki1·Takeshi Ando
J Artif Organs (2017) 20:377–380 DOI10.1007/s10047-017-0999-9
Case presentation
患者男,81岁,既往有慢性阻塞性肺气肿和重度吸烟史(4包/天,37年)。患者曾因充血性心力衰竭(纽约心脏协会心功能III级)三次入院,被当地心内科医生诊断为二尖瓣、三尖瓣重度反流以及阵发性房颤,其后患者至我院拟行手术治疗。超声心动图检查结果显示左心室扩张(舒张末期直径为61mm),收缩功能下降(射血分数为38%),重度功能性二尖瓣反流、三尖瓣瓣环扩张伴中度反流。我们拟为患者进行二尖瓣及三尖瓣修复术加迷宫手术。
The patient was an 81-year-old man whohad a history of chronic obstructive lung disease and heavy smoking (4packs/dayfor 37 years). He had three episodes of hospital admission due to congestive heart failure symptoms (NewYork Heart Association class III). Significant mitral and tricuspid regurgitations were identified by a local cardiologist as well as paroxysmalatrial fibrillation. He was then referred to us for surgery. Hisechocardiography showed left ventricular dilatation (end-diastolic diameter, 61mm) with depressed systolic function (ejection fraction, 38%), severe functional mitral regurgitation with leaflet tethering, and moderate tricuspid regurgitation with annular dilatation. He was diagnosed as a candidate formitral and tricuspid valve repair and the Maze procedure.
术中过程顺利。二尖瓣修复采用自体心包条加固后瓣、瓣环成形术,三尖瓣仅用瓣环成形术修复术。截取左心耳,并将射频消融联合冷冻消融应用于改良的双房迷宫手术。主动脉钳夹时间为168分钟,体外循环时间为214分钟,手术持续了7小时20分钟。
The patient underwent surgery uneventfully. The mitral valve was repaired by posterior leaflet augmentation using autologous pericardium and ring annuloplasty, and the tricuspid valve was repaired byannuloplasty only. The left atrial appendage was amputated, and the modified biatrial Maze procedure was conducted using a radiofrequency device andcryoablation. Aortic clamp time and cardiopulmonary bypass time were 168 and214 min, respectively. The surgery lasted 7 h and 20 min.
术后初期,患者的病情很平稳。在入住重症监护室(ICU)时,APACHE III(急性生理学及慢性健康状况评分)为60分,预期患者在ICU住院时间约为6天。序贯性器官衰竭评估(SOFA)评分为8分。术后第一天,患者因氧合良好予以拔管。动脉血氧分压(PaO2)与吸入氧浓度(FiO2)比(P / F比)为392 mmHg(图1)。胸部X线片显示未发现肺内浸润影(图2a)。然而,在第2天患者出现氧合差,需要无创正压通气。在第6天时患者高热并被诊断为肺炎。第7天时,患者重新插管。第8天时开始吸入一氧化氮治疗以使通气灌注不匹配最小化。痰培养结果为耐甲氧西林金黄色葡萄球菌,并开始使用万古霉素。在第8-10天时进行了类固醇脉冲疗法。虽然患者的P / F比从不到100mmHg暂时恢复到接近200mmHg(图1),但是患者的病情再次恶化,出现咳泡沫痰症状,胸部X线显示典型ARDS影像表现(两肺浸润阴影)(图2b),呼吸机条件提高[FiO2 =0.8,呼气末正压(PEEP) = 10cm H2O,气道峰压(PIP)= 26mm H2O]。第17-19天时进行了第二次类固醇脉冲疗法,但未改善患者病情。第18天时,因其P / F降至100mmHg以下(pH, 7.445; PaO2, 68.3mmHg; PaCO2,40.0 mmHg; FiO2, 1.0; PEEP, 10 cmH2O; and PIP,26mmH2O),患者SOFA评分增至12分。患者发热(体温38.3℃),白细胞计数升高至18440 /μl,C-反应蛋白11.50mg / dl。然而,血培养结果均为阴性,并且降钙素原水平不是很高0.15ng/ml。最重要的是,患者没有出现其他器官功能障碍的症状。患者在丙泊酚镇静下,神经系统无任何异常表现。在小剂量的肾上腺素和去甲肾上腺素的维持下,患者的平均动脉压稳定在81 mmHg左右,血小板计数为29.8×104 /μl。此外,患者的总胆红素从重插管后的3.6mg/dl 降至2.3mg/dl,肌酐从术后的2.12mg/dl降至1.01mg/dl,尿量超过3000ml/天。我们决定使用静脉-静脉ECMO模式,预防多脏器衰竭(MOF),希望使患者的肺功能恢复从而挽救其生命。
The patient’s postoperative course was initially smooth. Upon Intensive Care Unit (ICU) admission, his Acute Physiology and Chronic Health Evaluation III score was 60, predicting thelength of ICU stay to be approximately 6 days [7]. His Sequential Organ FailureAssessment (SOFA) score was 8 [8]. He was extubated the day after surgery with good oxygenation. Partial pressure of arterial oxygen (PaO2) to fraction ofinspired oxygen (FiO2) ratio (P/F ratio) was 392 mmHg (Fig. 1). Chest X-rayshowed no infiltration (Fig. 2a). However, he showed worsening oxygenation onday 2, requiring noninvasive positive pressure ventilation. He had a spikefever on day 6 and was diagnosed with pneumonia. He was reintubated on day 7.Administration of inhaled nitric oxide was started on day 8 to minimizeventilation-perfusion mismatching. Methicillin-resistant
staphylococcus aureus was detected fromsputum culture, and vancomycin was started on day 8. Steroid pulse therapy wasconducted on days 8-10. Although his P/F ratio temporarily recovered from lessthan 100 mmHg to approximately 200 mmHg (Fig.1), his condition once againdeteriorated, showing appearance of foamy expectoration and typical ARDS shadowon chest X-ray (Fig. 2b) with worsening ventilator support [FiO2=0.8, positive end-expiratory pressure (PEEP) = 10 cm H2O, peak airway pressure(PIP) = 26 mmH2O]. Second steroid pulse between days 17-19 wasconducted without improvement. On day 18, his SOFA score increased to 12 simply due to worsening P/F to less than 100 mm Hg (pH, 7.445; PaO2, 68.3mm Hg; PaCO2,40.0 mm Hg; FiO2, 1.0; PEEP, 10 cm H2O;and PIP, 26 mmH2O). The patient was febrile (temperature, 38.3℃)with an elevated white blood cell count of 18440/μl and C-reactive proteinlevel of 11.50 mg/dl. However, blood cultures were all negative, and the procalcitonin level was not very high at 0.15 ng/ml. Most importantly, the patient showed no other signs of organ dysfunction. The patient was sedated bypropofol without any abnormal neurological signs. His mean arterial pressure was stable at 81 mmHg with low-dose epinephrine and norepinephrine, and hisplatelet count was 29.8×104/ul. Additionally, his total bilirubinlevel decreased from 3.6 mg/dl after reintubation to 2.3 mg/dl, and his creatinine level improved from 2.12 mg/dl just after surgery to 1.01 mg/dl,with urine output of more than 3000 ml/day. We decided to introduce avenovenous ECMO system, expecting that lung recovery can save this patient and prevent multiple organ failure (MOF).
使用Seldinger穿刺方法分别在右侧股静脉和右侧颈内静脉插入20Fr和16Fr的导管。我们使用的是带有NSH肝素涂层的PCKC导管。体外膜氧合最初使用为MERA的离心泵和膜肺氧合器。在前7天因人工肺出现血浆渗漏导致我们不得不两次更换管路,在第25天时更换为带有X涂层(表面为泰尔茂公司专有涂层)的CAPIOX 离心泵和膜肺氧合器(泰尔茂公司,日本东京),预期能长期支持体外循环的运行。
The right femoral and right internal jugular veins were cannulated with a 20 Fr and a 16 Fr cannula,respectively,using the Seldinger technique. We used PCKC Cannulae with NSH heparin coating (SENKO MEDICAL INSTRUMENT Mfg. CO., LTD., Tokyo, Japan).Extracorporeal membrane oxygenation was initially induced using a MERA Centrifugal Pump NSH-R and a membrane oxygenator MERA NHP Excelung NSH-R (SENKOMEDICAL INSTRUMENT Mfg. CO., LTD.). Because we had to exchange the circuit twice due to plasma leakage from the artifcial lung in the first 7 days, the X coating (TERUMO’s polymer surface coating) system using a CAPIOX SL Centrifugal Pump and a CAPIOX LX Oxygenator (Terumo Corp., Tokyo Japan) was introduced onday 25, with prolonged support expected.
人工心脏的输出流量由最初的4.0 L /min,逐渐下降至3.0 L/ min。使用ECMO后患者的P / F比迅速改善至300 mmHg(图1)。然后应用肺保护策略机械通气(FiO2为0.40,PEEP为5 cm H2O,PIP为20 cm H2O)。未使用抗凝剂。
Pump flow of 4.0 L min was initially achieved, and gradually decreased to 3.0 L min. The patient’s P/F ratio quickly improvedto 300 mmHg after ECMO induction (Fig. 1). The ventilator was then set to alung-protective strategy with FiO2 of 0.40, PEEP of 5 cm H2O,and PIP of 20 cm H2O.Anticoagulation was not used.
使用ECMO后,患者的肺部情况仍逐渐恶化,主要表现使用吸痰(理疗)甚至使用俯卧位通气都不能改善。第20天时开始小剂量甲泼尼龙(0.5mg / kg)。第31天时进行了传统气管切开术。气管切开术后有效地吸痰使患者的肺部情况得到改善(图1),虽然手术部位没有明显的出血点,但气管切开部位周围仍不断渗血。我们诊断为弥散性血管内凝血(DIC),日本急诊医学学会DIC评分为4分(尽管输注了血小板,血小板计数还是降至7.9×104 /μL,纤维蛋白降解产物升至78μg/ ml)。考虑可能是ECMO诱导的DIC。然后,我们开始逐步撤除病人的ECMO,同时使用重组人可溶性血栓调节蛋白治疗DIC(自2015年7月以来已在日本正式批准用于DIC,报道称治疗有效且出血并发症少)。FDP迅速下降至12μg/ ml,没有继续出血。
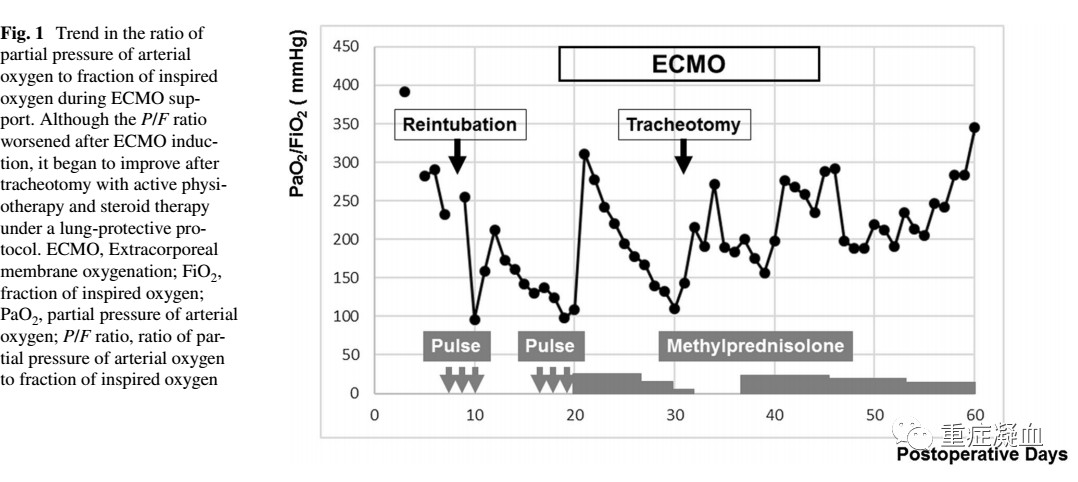
After ECMO induction, the patient’slung conditions worsened gradually, mainly related to ineffective sputumsuction (physiotherapy) even utilizing prone position.Low-dosemethylprednisolone (0.5 mg/kg) was started on day 20. Conventional tracheotomy was performed on day 31.Although his lung condition improved with effective sputum suction after tracheotomy (Fig. 1), bleeding around the tracheotomy site was complicated without apparent surgical bleeding site. He was diagnosed with disseminated intravascular coagulation (DIC) with the Japanese association for acute medicine DIC score of 4 (decreased platelet count of 7.9 × 104/μLdespite platelet transfusion and elevated fibrin degradation products of 78μg/ml). The cause of DIC was thought to be the ECMO support itself. We then proceeded to wean the patient off ECMO while managing the DIC using recombinant human soluble thrombomodulin(Recomodulin®;Asahi Kasei Pharma Corporation Ltd.,Tokyo, Japan), which has been ofcially approved for DIC in Japan since July 2015 and reported effective with less bleeding complications [9]. The FDP quickly decreased to 12 μg/ml, withoutprogression of bleeding.
第44天时,成功撤离ECMO,胸部X线显示肺部情况改善(图2c)。逐渐减少类固醇的剂量。ECMO撤离后,气管切开部位的出血自行停止,而且血小板的计数也迅速恢复。感染症状消失,第55天时停用万古霉素。第56天时停止吸入性一氧化氮治疗。ECMO撤离后,患者的病情缓慢而稳定地恢复,并在第65天时转入普通病房。第115天时,成功脱机,并在第141天时拔出气管套管。第172天时,患者能自己行走,并且不需要气管切开术后护理,转到普通的护理机构继续疗养。
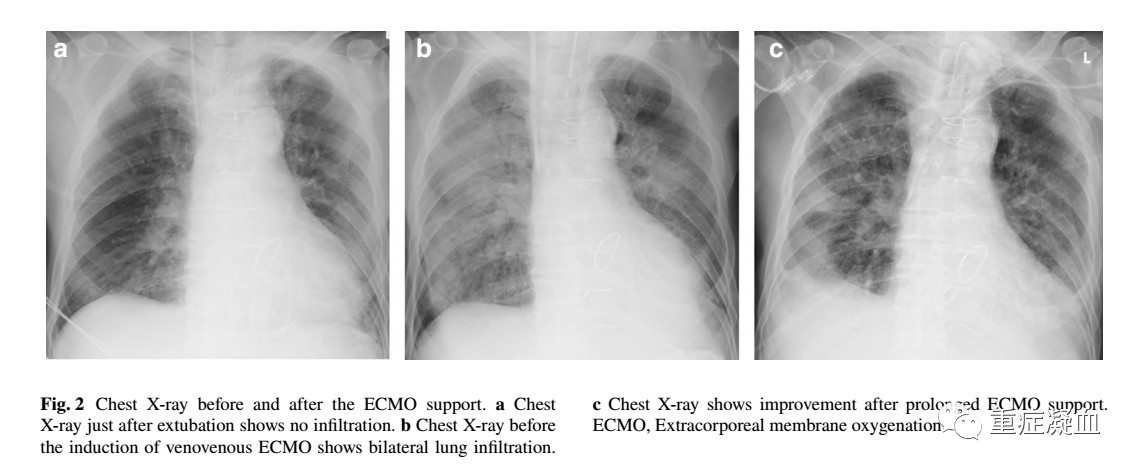 ECMO support was successfully terminated on day 44 with improvement in chest X-ray (Fig. 2c). Steroid dose was gradually decreased as well. Bleeding from the tracheotomy site disappeared spontaneously after ECMO termination, and was accompanied by quick plateletcount recovery. Signs of infection disappeared, and vancomycin was discontinued on day 55. Inhaled nitric oxide was discontinued on day 56.The patient’scondition showed slow and steady recovery after ECMO termination, and he was transferred to the general ward on day 65. He was weaned from the ventilator onday 115, and tracheotomy tube was removed on day 141. He was ambulatory and discharged to a nursing facility without tracheotomy on day 172
ECMO support was successfully terminated on day 44 with improvement in chest X-ray (Fig. 2c). Steroid dose was gradually decreased as well. Bleeding from the tracheotomy site disappeared spontaneously after ECMO termination, and was accompanied by quick plateletcount recovery. Signs of infection disappeared, and vancomycin was discontinued on day 55. Inhaled nitric oxide was discontinued on day 56.The patient’scondition showed slow and steady recovery after ECMO termination, and he was transferred to the general ward on day 65. He was weaned from the ventilator onday 115, and tracheotomy tube was removed on day 141. He was ambulatory and discharged to a nursing facility without tracheotomy on day 172


